Publications
Core Concepts and Trends in Iliopsoas Strains
Caroline Adamson Adrian, MSPT, CCRP Tamara Wolfe, BSPT, CCRP, GCFP
VCA Alameda East Veterinary Hospital, Denver, Colorado
Core stabilization is a developing concept in large and small animal physical therapy. A dynamic core stabilization program is an effective and important component of all comprehensive rehabilitation programs for the treatment of human low back pain. Trends in acute and chronic iliopsoas strain are revealing a remarkably high number of dogs presenting with spinal dysfunction and back pain. It is suggested that a dynamic core stabilization program, in addition to manual therapy, be incorporated in the treatment and prevention of canine iliopsoas strain with spinal dysfunction.
CORE STABILIZATION
The concept of core stabilization exercise may be defined as “the restoration or augmentation of the ability of the neuromuscular system to control and protect the spine from injury or reinjury.” Most exercise programs for the treatment of spinal pain focus on strength, endurance, and fitness as well as functional capacity training. These more general programs are most appropriate in the late stages of rehabilitation to increase general muscular support of the spine and are of benefit to the deconditioned patient. More recent research suggests that a key impairment in those with low back pain is one of motor control rather than just a lack of strength alone. The aim of core stabilization is to control pain and protect and support the spinal segment[s] from reinjury. This is accomplished by re-establishing and improving muscle control to compensate for any loss of segmental stiffness in the spine caused by injury or degenerative changes.
Strategies of core stability exercise may be divided into 2 components: restore control and coordination of the trunk muscles to ultimately improve control of the lumbar spine and pelvis; and restore the endurance and strength (‘capacity’) of those trunk muscles to help meet the demands of control of the spine and pelvis.
The first approach, control, is dependent upon the central nervous system (CNS) which determines the requirements of stability in order to plan and implement certain strategies in which to meet capacity demands. It is the sensory system that provides information about status of stability where stability is challenged by predicted control of the spine through an internal or external force [eg, forces used to generate movement of a limb]. The sensory system must also provide information about stability status through unexpected perturbations where the CNS must initiate trunk muscle responses to maintain stability.
The second approach, capacity, is fueled by the well- established Euler model which states stability of the spine is dependent on the contribution of muscle. If the lumbar spine is devoid of muscle, buckling failure will occur with a compressive load as small as 90 Newtons. This model suggests that the activity of muscles spanning the lumbar spine help to stiffen the intervertebral joints and maintain the spine in a mechanically stable equilibrium.
Thus, the goal of core stabilization exercise is to improve postural control, ensure appropriate muscular balance and joint motions, allows for expression of dynamic functional strength and improved neuromuscular efficiency throughout the entire kinetic chain. Many of these canine muscles that are required for spinal stabilization include the multifidus, transverse abdominus, obliques, transversospinalis, erector spinae, gluteals, latissimus, longissimus, iliocostals, serratus dorsalis, rectus abdominus, and iliopsoas. The body’s stabilization system must be functioning optimally to effectively use the strength, power, neuromuscular control, and muscular endurance that they have developed in their prime movers.
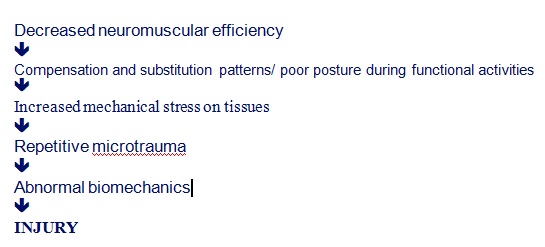
Structural changes due to disc disease, muscular changes such as poor endurance and weakness, or ineffective neuromotor control may all contribute to spinal instability and back pain. The biomechanics of those with nonspecific low back pain differ from those without back pain. Neuromuscular control combines postural alignment and stability strength to allow the body to decelerate gravity, ground reaction forces and momentum at the right joint, in the right plane of motion, at the right time. If this system is not efficient, it will be unable to respond to the demands placed on it during functional activities. As the efficiency of the neuromuscular system decreases, the ability of the kinetic chain to maintain appropriate forces and dynamic stabilization decreases significantly. Thus, if extremity muscles are strong and the core is weak, then there will not be enough force created to produce efficient movements. A weak core is a fundamental problem of inefficient movements that may lead to injury. An illustration of the potential for injury may be described in the diagram below.
Orthopaedic Practice Vol. 20;3:08
INJURY ILIOPSOAS
This muscle, a fusion of the psoas major and the iliacus, originates on the transverse processes of the lumbar vertebrae 2 to 4 in addition to the ventral and lateral surfaces of lumbar vertebrae 4 to 7. The iliopsoas attaches to the lesser trochanter of the femur. Several articles as early as 1995 have reported traumatic injury to the iliopsoas muscle as evidenced by CT, MRI, and ultrasound.
The article by Fitch, Montgomery, and Jaffe continues to explore the detrimental effects of a muscle strain to include the process of inflammation and edema that will occur with acute trauma. The muscle contractile force is thus affected by a strain injury and normal histology is not restored. Scar tissue will persist in the muscle with the potential for repetitive trauma and continued tearing of the scar tissue if not treated. Prolonged immobilization will result in irregular muscle fiber patterns, further decreasing tensile strength as the muscle is replaced with fibrotic scar tissue.
Length of time of the iliopsoas strain also appears to determine outcome of treatment. Dogs with acute injuries of less than one month responded well to rest, restricted activity, and nonsteroidal anti-inflammatory medications. However, those dogs with clinical signs of greater than one month responded poorly.
TRENDS IN ILIOPSOAS STRAINS
In the past 8 months, data have been collected on dogs diagnosed with iliopsoas strain by 2 board certified surgeons. Trends in these data, documented by 2 physical therapists, include a limitation in active spinal and pelvic extension and rotation with functional activities. Moderate to severe muscle spasms have been evident in the lumbar musculature, and, in more severe chronic cases, have continued into the thoracic spine as far as the scapulae. In the areas of muscle spasms, decreased spinal motion in extension has been documented, in addition to a lack of spinal rotation and side bending. Pain, as verified by vocalization, pressure avoidance on palpation and muscle guarding (muscle spasm, tightness and sudden contraction along perispinal musculature) on dorsal palpation and rotation of spinal segments, has also been documented. These are possible correlations with what is seen clinically in dogs with iliopsoas strain, however, there are no current objective data to support these links.
As illustrated with the concepts outlined above, human physical therapy has recognized the relationship between weak core muscles causing decreased spinal stabilization that reduces structural support. In turn, this allows the musculature to be more prone to injury. Could there be a correlation between spinal dysfunction and iliopsoas strain in the dog? If so, where does the correlation lie? The challenge thus becomes pursuing the objective data necessary to prove or disprove these concepts of core weakness and their potential relationship to canine iliopsoas strains.
RESOURCES
1. Stubbs NC. Functional anatomy and dynamic stability of the thoracic and lumbopelvic region in relation to equine back pain. Proceedings, 4th International Symposium on Rehabilitation and Physical Therapy in Veterinary Medicine, 2006.